Registered dietitian Maiya Hogan shares practical tips for grocery shopping, reading nutrition labels, and making heart healthy choices after transplant. A helpful guide for anyone looking to support long-term heart health through everyday habits.
Tips and Tricks:
Healthy eating does not have to be complicated. Small swaps, like choosing lower sodium options and paying attention to labels, can make a big impact. You can also rinse canned food products like beans and vegetables before using them. Even low sodium versions can have extra salt that rinses off quickly under running water.
Making your own dressings is an easy way to control ingredients and avoid extra salt. For ideas, explore this simple dressing guide: https://www.gimmesomeoven.com/salad-dressing/
The proposed Living Donor Protection Act (LDPA) of 2025 (S.1552 / H.R.4583) is bipartisan federal legislation introduced in 2025 to protect living organ donors. Protections like the LDPA are essential to helping reduce the national transplant waiting list, which currently includes more than 100,000 individuals. Such legislation may encourage more people to consider becoming living organ donors for those in need of life-saving kidney and liver transplants.
Key Aspects of This Legislation
Insurance Protections:
Once enacted, insurance companies would be prohibited from discriminating against living organ donors—this includes denying coverage, limiting coverage, or charging higher premiums simply because someone is a donor.
Job Security:
When the law is (hopefully) in effect, recovery from organ donation surgery would be covered under the Family and Medical Leave Act (FMLA). This means donors will be able to take unpaid leave while recovering, with job protection to ensure they can return to work.
Status and Next Steps
Current (Federal*) Status:
on February 26, 2026, the LDPA advanced through the Senate Committee on Health, Education, Labor, and Pensions (HELP), moving it one step closer to becoming federal law.
On March 11, 2026, the LDPA was reported to the full Senate.
Next, the legislation will be debated on the Senate floor, followed by a final vote after any amendments are addressed. If approved by the full Senate, it must be reconciled with the House version before being sent to the President, who will either sign it into law or veto it.
Call to Action
We can all reach out to our representatives to ensure that LPDA becomes law. Our voices matter. Every day, people die while waiting for a life-saving transplant.
*There are also state-level laws that provide protections for living organ donors.
New platform supports patients with chronic kidney disease and dialysis through connection, education, and peer support
POMPANO BEACH, Fla., March 12, 2026 /PRNewswire/ — Today, on World Kidney Day, Patient Care America, a premier renal healthcare provider specializing in precision medicine nutrition support and clinical solutions for kidney disease patients, is proud to announce the launch of KidneyLyfe.com, a safe, moderated place where people living with kidney disease can connect online, feel supported by peers, and share experiences with others who face similar challenges.
KidneyLyfe was created to address the isolation many patients experience by offering a safe, supportive online space where individuals can connect with others who understand their journey, access trusted education, and feel more empowered in their care. The platform is designed for patients at every stage of kidney disease, as well as care partners supporting loved ones.
“This launch reflects our commitment to putting the patient first in everything we do,” said Philip Keough, President & CEO of Patient Care America. “KidneyLyfe is designed around the real needs of people living with kidney disease, supporting individuals as active participants in their care.”
Through KidneyLyfe, members can access:
- One‑to‑one connections with fellow patients who share similar experiences;
- Discussion forums to exchange insights, ask questions, and find peer support;
- Podcasts, blogs, and webinars featuring real patient stories and expert perspectives; and
- Educational resources that extend learning beyond the clinic, informed by both lived experience and clinical expertise.
“Experiencing chronic illness is isolating and finding peer support is often difficult through traditional channels,” said Karin Hehenberger, MD, PhD, Founder of Lyfebulb, a Patient Care America company. “That’s why we created KidneyLyfe – to offer a supportive online space where patients can connect, learn, and feel empowered. This platform is about bringing people together, sharing real experiences, and making sure no one faces this disease alone.”
KidneyLyfe is part of Patient Care America’s broader commitment to advancing patient‑centered care by developing solutions that support individuals with kidney disease beyond the clinic and empower patients in their healthcare decisions.
Patients and care partners are invited to join the community at www.kidneylyfe.com.
About Patient Care America
Patient Care America is a premier renal healthcare provider specializing in precision medicine nutrition support and clinical solutions for kidney disease patients. PCA offers evidence-based therapies such as IDPN (Intradialytic Parenteral Nutrition) and IPN (Intraperitoneal Nutrition) to help manage malnutrition and improve clinical outcomes. Backed by published research, its therapies are trusted by nephrology teams and dialysis clinics nationwide. PCA also offers bundled prescription medications, streamlining delivery and supporting improved medication adherence. PCA advances its commitment to supporting patients beyond the clinic with the patient empowerment tools delivered through its Lyfebulb platform.
About Lyfebulb
Lyfebulb is a Patient Care America company focused on empowering people living with chronic diseases through education, innovation, and connectivity. Lyfebulb developed and operates both TransplantLyfe.com and KidneyLyfe.com, community‑driven platforms that empower patients to achieve optimal health outcomes, as well as an app to help patients keep track of symptoms and medications, called TransplantLyfe365.
MEDIA CONTACT:
Karin Hehenberger, MD, PhD
Chief Medical Officer
Patient Care America
Karin@Lyfebulb.com
+1 917 227 8523
SOURCE Patient Care America

When I was 18 years old, I started having strange symptoms: body aches that never went away, a really hard time breathing, and a heart that would skip beats or feel like it was pounding so hard that it would move my entire body. After several misdiagnoses, I was finally diagnosed with end-stage heart failure from a rare genetic condition called left ventricular noncompaction cardiomyopathy. I needed emergency surgery that night to place an Impella to help my heart pump, but it failed. I was placed on another form of life support called ECMO, which would circulate my blood for me.

I was placed on the transplant list as Status 1A to try to get a heart for me as soon as possible. In the two weeks of waiting for my transplant, I was placed on a ventilator because my lungs were filling with fluid. I was dying, and I was dying quickly. I had also sustained a spinal stroke while waiting for my transplant. Finally, I received my heart on March 21, 2022. I remember being rolled into the OR, barely conscious, and being asked, “Do you have any questions before we start?” I asked the transplant surgeon if I was going to die. I don’t remember his answer, only his calm kindness.

When I was a kid, I was kind of shy, more of a quiet observer type. It wasn’t that I never had anything to say; it was that I was afraid of how I would be perceived. I never really knew what I should say. I kept my words safe inside of me for most of my life. In the two days after my transplant surgery, I would not speak or write notes. The words were once again stuck inside of me, just as they were when I was a kid. I knew I wanted to say something; nothing could encapsulate what I was thinking.

In the beginning months after my transplant, everyone told me I was lucky. But I was stuck at this strange intersection of not knowing the magnitude of what I survived, not knowing what it meant to be lucky, being so immensely thankful to be alive, and questioning why everything I thought I had planned for my life had been turned upside down.

After being intubated for a while, my voice sounded foreign to me. I have never been a good or strong singer, but my hum became breathless.
My laugh had always been loud and sometimes obnoxious, but when it fell silent, I quickly realized I missed it more than anything. I had a new body that I didn’t recognize and a new rough idea of a life plan that did not yet feel like my own. There was one night, soon after coming home from rehab, when I was taking my vast number of nightly pills, and I broke down crying.

My family looked at me like I was crazy at first; I think they were trying to understand how the feeling of luckiness could be overpowered by another, more complicated feeling—grief. As someone who always loved the freedom of no structure, I felt so exhausted by having to follow this new, strict routine.

I had this deep feeling in my soul that every cell of my being had changed—that I would never walk again, that I would never just go back to who I was before. It posed a new question: What if I was always meant to end up this way? What if I was meant to have a new laugh and voice, a new perspective, a new body, a new future?
What if this would teach me how to say all of the things I feared saying for my entire life? What if it is actually better that I cannot go back to who I was before? I did not want it all to mean that what happened to me was cruel or unfair. I desperately wanted to shake hands with my grief, call it a truce, and somehow live in peace with its shadow so that it would not dim my life forever.

I began unpacking everything that transpired leading up to my transplant. I wanted to take it all apart piece by piece to inspect it, to try to understand the luckiness that found me. My sister had taken detailed notes throughout my arrival at the hospital, all the way until the week after my transplant surgery. She and my mother saved all the notes I wrote while on a ventilator, when my writing was barely legible at times. I vividly remember being frustrated while writing each one because the words never came out the way I wanted.

From all the pain and sleep medications I was on, I didn’t know how to write normally—some letters and words were so tiny or squished together that they made no sense. I read them so many times that the memories etched themselves into me. Reading that your family was told to make death plans for you if a heart didn’t rescue you in a few days is something you can never forget.

The memories of the ICU tug at me sometimes, and I often can’t tell if it is from the fear that some imaginary clock is ticking against me or if it is because I feel I haven’t thanked that room enough. It can freeze me for moments in time, holding me hostage. I wake in the middle of the night after having dreams of memories I try to suppress in my waking life—the ones that are too staggering to face.

Though there is something else I read in my sister’s notes, which she wrote the day after my transplant surgery, that has not left me either: “I’m sitting in the chair in the sky lounge and don’t have to sit and wonder if Carrots will get a heart or not.” If for no grander reason than living another day where my sister calls me Carrots, living another year where my mother squeezes my hand during quarterly bloodwork tests, or laughing my new laugh with my best friends, I think it is still worth it.

As I write this, the geese are loudly migrating over the Lehigh Valley in Pennsylvania, where I live. I wonder if they are flying back to places they feel they did not thank enough—if they are driven by their memories too. I think about the woman who saved my life. I tell everyone about her, even strangers. I tell them how she is the ink of my name when I dot the “i” in Caroline with a heart. How I carry her like a second soul. How she finds me in every poem I write at 2 a.m. I wonder a lot about my lucky Penny—if her spirit returns to those thankful places, to the creek or grass barefoot.

If she could be out there on the clouds the geese are flying under, arms outstretched in fields of cotton sky. If she had a clear view of the last full Blood Moon in March 2025 and thought that it looked like the magnificent heart, she gifted me.
Most days, I wake up with the sun shining in my eyes, and occasionally I wish my blinds would close tighter, but I am reminded of a random quote I read online: “I opened two gifts this morning; they were my eyes.” I believe the third gift is my heart, beating with me, no matter the fear that creeps in or the memories that feel like a confusing illusion. I say that I am lucky, and I feel that I am.

Caregiving. Most of the time, this word conjures images of grown children caring for aging parents, or seniors caring for seniors. Sometimes it brings to mind younger people caring for a loved one with cancer. One image most people don’t consider is caregivers for chronic conditions. We are unsung heroes.
It comes with mixed feelings. Our loved ones are dying… but slowly. Some can even be restored to “normal” with a transplant, if everything goes well. Others move through stages, gradual or abrupt, that require constant adjustment and flexibility. The traditional definition of a caregiver doesn’t always apply. In conversations, we may feel guilty about identifying as caregivers. But our role is long, arduous, and often misunderstood.
We are caregivers.

We navigate care. We become armchair experts, hyper-attuned to any nuanced change in our loved one. We move through endless lists of specialists. We get listed for transplant at this hospital, or that hospital — sometimes five different ones. We become disciplined and relentless in medication management, movement, emotional regulation, and advocacy. We live constantly on the razor’s edge between compassion and militancy to keep our person alive and thriving.
We are caregivers.
We need support, love, inclusion, respite, and care of ourselves. We deserve recognition for the work we do — even if we don’t seek it. We deserve community and safe spaces to connect with others, to talk or not talk about our experiences, and to remember what it feels like to be a full human being independent of caregiving.
I urge you to find spaces like this for yourself, so you can continue the fight.
Because:
WE ARE CAREGIVERS.
“Improve Your Care Through Medication and Symptom Tracking” is the second webinar in our 2026 educational series. Maiya Hogan, MS, RDN, CD, CNSC, sat down with Dominika Woch, a kidney transplant recipient and Community Manager for KidneyLyfe and TransplantLyfe, to talk about how keeping track of medications and symptoms can make a real difference in your care. The session explores how using a tracking system, like the TransplantLyfe365 app, can help you stay organized, understand your health changes, and feel more confident during appointments. They also share tips on how tracking can support better communication with your care team and help you become a stronger self‑advocate.

August 22, 2022, changed my life. My now-fiancé and I had only been dating for two and a half months when he was diagnosed with end-stage renal failure. To say our lives were turned upside down is an understatement. We were still learning about each other when we suddenly found ourselves facing kidney failure — he as the patient, and I as the caregiver.
Coming from a background of service as a Veteran, it was a no-brainer that I would tackle this journey head-on. And oh, what a journey it has been — a rollercoaster of emotions, triumphs, and setbacks all at once.

In the early stages of a relationship, every day usually brings new discoveries, laughter, and sometimes awkward moments. For us, those moments were suddenly magnified by a medical crisis. We were no longer just exploring favorite foods or binge-worthy shows; we were navigating lab results, dialysis schedules, and endless doctor appointments.
My military background instilled in me a deep sense of duty, discipline, and service. But nothing could have prepared me for the emotional intensity of watching someone I love fight for his life. Overnight, I became his advocate, nurse, nutritionist, and emotional anchor. There were days when the weight of responsibility felt overwhelming, and nights when fear crept in uninvited.
Being a caregiver means embracing a whirlwind of emotions: grieving for the life we once imagined, hoping for better days, feeling frustrated by setbacks, and holding profound gratitude for even the smallest victories. This journey has revealed depths of empathy and love I never knew I possessed. We have grown together in ways I never could have imagined, finding joy in quiet moments and celebrating every step forward.

Our story is not one of perfection, but of perseverance and partnership. Every challenge has been a lesson. Every triumph has been a reason to hold each other closer.
If you are reading this as a fellow caregiver, know that you are not alone. Your strength and compassion matter, even on the hardest days. Remember to care for yourself as fiercely as you care for your loved one. As difficult as it may be, this is the number one rule.
The journey will always be unpredictable, but your courage lights the way.
Thank you for joining me as I continue to share our story — one day, one triumph, and one setback at a time. I currently reside in California and have included both local and national caregiver resources.
National and Online Caregiver Resources
- Family Caregiver Alliance
- In-depth information, personalized support, CareNav dashboard, and resources in multiple languages.
- Family Caregiver Alliancecaregiver
- Caregiver Action Network
- Free education, peer support, and resources for family caregivers, including a Caregiver Help Desk and condition-specific guides.
- Caregiver Action Networkcaregiveraction
- National Institute on Aging – Caregiving Toolkit
- Evidence-based articles, infographics, publications, and videos for caregivers.
- NIA Caregiving Toolkitnih
- AARP Caregiving Support Groups
- Guidance on finding the right support group, both online and in-person, with tips for connecting with others who understand your journey.
- AARP Caregiving Support Groupsaarp
- Family Caregivers Online
- Articles, webinars, support groups, and a resource directory for caregivers nationwide.
- Family Caregivers Onlinefamilycaregiversonline
- VA Caregiver Support Program
- Specialized support for caregivers of veterans, including counseling, education, and financial planning.
- VA Caregiver Support Programva
- Comprehensive List of Support Groups
- A roundup of 22 online and in-person caregiver support groups, including those for specific conditions.
- 22 Remarkable Caregiver Support Groupsseniors
My name is Sam and I’m an extremely lucky, completely blessed, and eternally grateful heart recipient and survivor since April 2015. Like most organ recipients, I too hadn’t imagined ever needing a transplant but now, almost 11 years post-transplant, I’m not just surviving, but thriving. My first-hand experiences have allowed me to listen, observe, and become well-educated about all things Organ Donation and Transplantation over the years. I’ve become a fierce advocate/voice for transplant patients/recipients and others who may be connected to transplantation, both as an individual contributor and through other advocacy entities/organizations. I’m not an expert in this arena by any means, but I try to be aware, diligent, and be well-informed about things going on in this ever-evolving space.
I feel it’s important for all of us in the larger transplant community to be involved and invested in our collective care, which is why in upcoming newsletters, I plan on providing information about relevant media stories, advocacy efforts, and proposed legislation.
If anyone has relevant items/information to share, your content could possibly be featured in this section of the newsletter! Kindly contact me by sending a direct message to my profile on TransplantLyfe. Alternatively, please don’t hesitate to email me at sam@transplantlyfe.com.
——
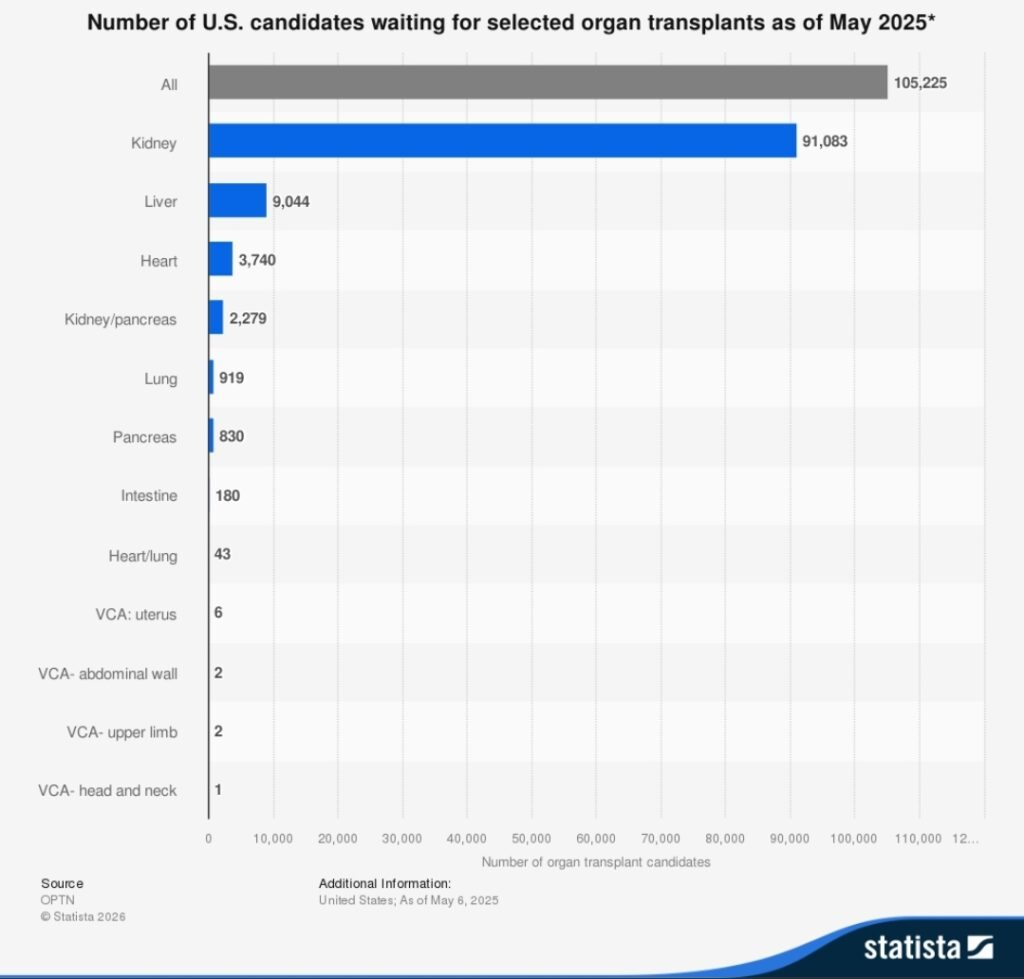
At present, in the United States, there are over 90,000 people waiting to receive a life-saving kidney transplant. The demand for kidneys far exceeds the supply, leading to long waits, sometimes more than 5 years. Over the years, there have been some policy changes and efforts to improve data, equity, and transplant rates. However, the waitlist continues to grow because not enough folks are able to be transplanted due to the shortage of organs. Additionally, there’s been a troubling decline in deceased donor transplants in the last 12 months. Consequently, the need for more donors is even more critical. One viable solution to increase the donor pool is to encourage more living donors to step forward and donate a kidney to save a life. To that end, there has been some great work to introduce legislation that could help mitigate the organ shortage situation.

One such proposed legislation is the (EKDA) End Kidney Deaths Act (H.R. 2687) which is a ten-year pilot program that will provide a refundable tax credit of $10,000 each year (for a total of $50,000 over 5 years) to living kidney donors who donate a kidney to save the life of a stranger, by way of a non-directed donation. A non-directed kidney donor is someone who donates without having a specific recipient in mind when donating a kidney. This one selfless act could even start a “chain” of transplants which would potentially help several recipients. These non-directed kidneys will go to those on the National Waiting List who have been listed for the longest. The hope is that by the 10th year after the passage of the EKDA, up to 100,000 Americans who had been suffering on the waitlist will instead have healthy kidneys. (Also, over this period of time, taxpayers will have saved several billions too.)
To learn more information about EKDA, you can visit its Congress.gov listing, and/or https://www.endkidneydeathsact.org/., and watch this educational video. Interested advocates can also sign this petition.
#Advocacymatters #PatientVoice #livingdonorssavelives #shareyourspare #beanorgandonor #bealivingdonorhero

Twelve years after my kidney transplant, it’s impossible to ignore both the freedom it’s given me but also one of its most serious challenges: skin cancer. With a family history of cancer and lifelong immunosuppression, I knew the risk was real.
After an initial diagnosis in 2021 and back-to-back diagnoses in late 2025/early 2026, I felt compelled to share my journey with biopsies, Mohs surgeries, and wound complications so others can benefit from my experiences.
Ultimately, here’s what I learned:
Stay vigilant about checking your body. Trust your gut. Don’t ever settle for appointments that seem eons away. While skin cancer is a common transplant experience, it’s valid to express displeasure if it happens to you. It may happen again. You can complain that time too. Your gratitude for a life-saving transplant is in no way diminished by being angry (or frustrated) you may have to endure skin surgeries, physical pain, stress, and medical bills. You’re not alone. The TransplantLyfe community is here for you.
This is my story…

——
Recently, when driving back home from an evening concert in New York City, I reflected on my health and all the gifts my kidney transplant has afforded me in the almost twelve years since my surgery.
The ability to enjoy a night out with friends, experiencing my favorite pastimes (live music) without having to worry about rushing home early to plug into a peritoneal dialysis cycler for 10 hours, is certainly at the top of that gratitude list.
However, the following morning, in stark contrast to the previous night’s fun, I woke up very early for a not-so-pleasant aspect of transplant life: addressing skin cancer (again).
I’m currently 39 years old and my first experience with the dreaded “c”-word occurred in middle school when my father required invasive surgery to remove a melanoma on his arm. At the time, there was concern it had spread to his lymph nodes. Thankfully, the tumor was fully excised and Dad was OK. In the years since, he faced numerous instances of skin cancer, many of which involved Moh’s Surgery to resolve. (More on this highly effective removal technique later.)
When I received my living donor transplant from a close friend in 2014, I was told about the heightened risk of skin cancer due to the immunosuppressive drugs I would be taking for life. When factoring in family history, skin vigilance had to become an important part of my overall routine. Hats and high-SPF sunscreen became staples of my summer. I started seeing a dermatologist once a year for full-body screenings and tried my best to keep mental track of anything on my body that seemed off. Occasionally, some skin lesions such as actinic keratoses were frozen or burnt off just to be safe and to ensure these pre-cancerous conditions didn’t evolve.

In May of 2021, 7 years post-transplant, I noticed a small, dime-sized mark on the front of my hairline. Initially thinking it was just dry skin, I applied cream and observed it over the course of a few days. Nothing changed and my gut felt that something was wrong. I called my dermatologist who unfortunately was booked out about 8 weeks. I took the next available appointment on June 28th, we biopsied the spot via a tiny surgical cut, and on July 4th weekend I received a call noting the sample was a basal cell carcinoma. My first-ever Moh’s Surgery was scheduled for the next morning, and I was told to bring a book or something to occupy my time as the procedure could take upwards of 3 hours.

Moh’s Surgery involves numbing the area with local anesthesia followed by extremely precise surgical removal of tissue, which is then viewed under a microscope to detect cancer cells along the edges. No cancer cells, no more surgery. If cells are present at the edges, it’s time for more cutting. The wound is commonly sutured closed or cosmetically restructured using skin grafts or synthetic skin substitutes, depending on the location and size of the gap. Moh’s is highly effective for skin cancer, with success rates as high as 99% according to Johns Hopkins Medicine.
While I was very grateful the cancer was gone, I was still annoyed it took me weeks to get a proper office visit. After doing some online research, I found another clinic, which was highly rated, took my insurance, and even offered night hours and same-day appointments. I never returned to my prior provider.
Fast forward to the Fall of 2025, when I noticed a small tan colored spot just above my sideburn. My current dermatologist had me come in right away; the spot was frozen, and a few weeks later, it was out of sight and mind. Until it wasn’t. By December, the spot began crusting again and a biopsy confirmed the presence of a basal cell. I opted for Moh’s right away, pre-holidays. I forgot how much the local anesthesia needles hurt when entering the skin. I was quickly reminded of how the fresh incision felt a few hours later once the meds wore off. The sutures on the side of my head were TIGHT and sleeping was very uncomfortable. On New Year’s Eve, we removed the sutures, closing the door on that situation, and randomly biopsied a bleeding spot on my leg, which I initially thought was a minor cut.
The first week in January 2026, I had a voicemail from the dermatologist about “the results” from my leg. Since they didn’t leave good news on my line, I assumed the obvious: more cancer. Sometimes I hate it when I’m right.

The leg biopsy site wasn’t healing well, likely due to me being immunocompromised, but after a few days of topical creams, on January 15th, I had Moh’s for the second time in under a month. This spot was on the shin of my left leg. Same painful needles, same rude awakening hours later when the numbing meds wore off. Sleeping was OK but standing up and feeling the blood flow to the wound was OUCH.

On January 18th, still reeling from the pain in my leg, I woke up to tons of blood on my pillow. Despite my head sutures having been removed weeks prior, the center of the wound reopened exposing a gaping hole. This is known as wound dehiscence. It can happen even with a perfect suture job due to a multitude of factors. Thankfully, no infection was present.
On January 19th, the wound was re-sutured, and I was back to bandages and the TIGHT pain. We agreed to leave these stitches in longer than usual and will do the same with my shin sutures.
While more cancer in my future is uncertain, all I know for sure is that I will be going to another concert next week.
“A Practical Guide to Achieving Your Health Goals” kicked off the TransplantLyfe University Webinar Series. Dr. Karin Hehenberger, Lyfebulb Founder and a kidney‑pancreas transplant recipient, was joined by registered dietitian, Maiya Hogan, MS, RDN, CD, CNSC. Together, they explored why setbacks are common, especially in the transplant community, and how reframing them can keep individuals motivated rather than discouraged. The session equipped participants with practical strategies to set achievable goals, stay realistic, and confidently adjust or level up their goals over time.